
Shoulder Arthroscopy in Turkey
Contents:
- What is Shoulder Arthroscopy (Closed Shoulder Surgery)?
- Shoulder Arthroscopy (Closed Shoulder Surgery) and Shoulder Fiber Tear (Video)
- Shoulder Fiber Tears (Rotator Cuff / Cuff Tears)
- How Does Shoulder Fiber Tear Happen? / What Causes Shoulder Fiber Tear?
- Who Gets Shoulder Fiber Tear (Rotator Cuff / Cuff Rupture)?
- How to Diagnose Shoulder Fiber Tear (Rotator Cuff / Cuff Rupture)?
- What is the Treatment for Shoulder Fiber Tear? (What is the Treatment for Rotator Cuff Rupture?)
- What Happens If Shoulder Fiber Tear Is Not Treated? (What Happens If Rotator Cuff Rupture Is Not Operated?)
- How is Shoulder Fiber Tear (Rotator Cuff / Cuff Rupture) Surgery Performed?
- Closed (Arthroscopic) Shoulder Fiber Tear Surgery
- When Can I Use My Arm After Closed (Arthroscopic) Shoulder Fiber Tear Surgery?
- Shoulder Dislocation (Shoulder Joint Instability)
- What are the mechanisms of shoulder dislocation?
- What is the Treatment for Shoulder Dislocation?
- My Shoulder Dislocated and Then They Fixed It, What Happens Now?
- What Happens If I Don't Have Shoulder Dislocation Surgery?
- How Does Shoulder Dislocation Surgery Happen?
What is Shoulder Arthroscopy (Closed Shoulder Surgery)?
Closed joint surgeries (arthroscopy) are an accepted method that has been frequently used among orthopedic surgeons in the last 30 years. In arthroscopy, holes are made with small incisions around the joint. The operation is carried out in a closed manner by inserting cameras and tools into these holes. This procedure provides us with many advantages such as less bleeding, fewer wound healing problems, faster recovery and faster return to daily life.
Today, many shoulder joint-related problems such as shoulder fiber tears (rotator cuff / cuff tears) and shoulder dislocations (instability) can be treated with a closed (arthroscopic) method.
Shoulder Arthroscopy (Closed Shoulder Surgery) and Shoulder Fiber Tear (Video)
Shoulder Anatomy
One of the most important joints necessary for a person to continue his life independently is the shoulder. The shoulder joint is the joint of the body with the greatest range of motion.
A normal shoulder joint movement angles;
- Abduction 160 degrees,
- Adduction 50 degrees,
- Flexion 180 degrees,
- Extension 60 degrees,
- External rotation is 90 degrees in neutral and abduction,
Internal Rotation is about 45 degrees in neutral and 90 degrees in abduction.
In daily life, we need at least 150 degrees of shoulder flexion when combing hair, at least 50 degrees of shoulder flexion to use a spoon and fork, and almost full shoulder internal rotation to get dressed and undressed.
The shoulder joint basically consists of two bones. These are humerus and scapula. However, more than two bones participate in shoulder joint movement. These; humerus, scapula, clavicle, sternum and lateral costal surfaces. There is a complex of joints between these bones. These joint complexes function during shoulder joint movement. These joints; sternoclavicular joint, acromioclavicular joint, glenohumeral joint and scapulatoracic joint, and these are accompanied by the subacromial region. When evaluating all the shoulder pathologies, it is essential to consider these joints as a whole.
The anatomy of the shoulder area is relatively more complex than other parts of the musculoskeletal system. The learning curve takes a little more time. To make it easier to understand shoulder anatomy, we can divide it into superficial and deep.
Superficial Shoulder Anatomy
Superficial shoulder anatomy can be understood by visual (inspection) and manual (palpation) examination. We can examine the superficial anatomy of the shoulder by roughly dividing it into 3 regions. Front, back and upper area.
When we look at the frontal area, the bone can be examined manually by examining the sternum, collarbone (clavicle), epaulette bone (acromion), coracoid (crow nose) protrusion and the joints and ligament structures formed by these bones among themselves. From the soft tissues, the pectoralis major, the anterior part of the deltoid muscle and the deltopectoral groove formed by these two can be examined manually.
When viewed from the back, the bony structures such as the protrusion of the shoulder blade (spina scapula), the inner edge of the shoulder blade (scapula) and the posterior corner of the epaulette bone (acromion) can be seen and examined manually.
When viewed from above, the collarbone (clavicle) and epaulette bone (acromion) are fully visible and examined from inside to outside.
Deep Shoulder Anatomy
Deep anatomy can be examined more easily by dividing it into three parts: external, middle and internal.
In the outer layer; It includes the deltoid muscle. The deltoid muscle is the most important and strongest muscle of the shoulder. Its nerve is the axillary nerve, and its main feeding artery is the posterior humeral circumflex artery. The deltoid muscle is the main muscle that causes abduction and elevation (opening the arm to the side) of the shoulder joint. During the movement of opening the arm to the side, the front and middle fibers of the muscle are more active. It has a critical role in ensuring the stability of the shoulder joint.
Another structure located in the outer layer is the pectoralis major muscle. It is the largest muscle of the anterior chest wall. It is the main muscle that makes the arm move inwards by bringing it closer to the body. The place where it is attached is important for shoulder surgeries because it is in close proximity to the groove (bicipital groove) where the long head of the biceps muscle passes.
The deltopectoral space is a space we use when approaching the shoulder from the front during shoulder surgeries. It is between the deltoid and pectoral muscle. A vein called the cephalic vein passes through it. When we go one layer deeper than the deltopectoral gap, we see the middle layer structures.
In the middle layer; There is the coracoid (needle nose) protrusion, the conjoint tendon attached to it, and the pectoralis minor muscle (small chest muscle).
The coracoid process is the part of the shoulder blade that extends forward. The word coracoid can be translated into Turkish as crow nose or crow nose. This name was given by resembling a crow's beak to this structure. The short tendon of the biceps muscle, coracobrachialis muscle and pectorlis minor muscle are attached. The short head of the biceps muscle (biceps) and the coracobrachialis muscle attach together to the coracoid process. The structure formed by these two muscles just before they attach to the coracoid process is called the conjoint tendon. When we go one layer deeper than the cone tendon, we can evaluate the structures included in the inner layer.
In the inner layer; The rotator cuff is one of the most important structures of the shoulder joint. The disorder popularly known as shoulder fiber tear is the tear of the rotator cuff in this layer.
Rotator Cuff / Rotator cuff can be defined as a collection of muscle tendons formed by 4 muscles. These muscles;
- Subscapularis muscle,
- Supraspinatus muscle,
- Infraspinatus muscle,
- Teres Minor muscle.
The common feature of these muscles is that they attach to the head of the upper arm bone (humerus), starting from the shoulder blade (scapula). They surround the area called the head of the humeus from the front, top and back.
Subscapularis muscle; It is the only rotator cuff muscle located in front of the shoulder joint. It is the strongest and largest among the rotator cuff muscles. While the upper fibers of this muscle (upper 2/3) adhere to the humerus by forming a tendon structure, the lower fibers (lower 1/3) adhere to the humerus as a muscle without forming a tendon. The function of this muscle is to ensure the stability of the shoulder joint in the front (preventing forward dislocation of the shoulder) and to make the arm rotate inwards.
Supraspinatus muscle; It is the muscle most commonly torn in the shoulder joint. It is located at the top of the shoulder joint. When shoulder fiber tear is mentioned, it is thought that this muscle is torn. Its function is to open the arm to the side. It makes this movement together with the deltoid muscle. Participates in the movement of opening the arm up to 90 degrees. It does not participate in arm opening movements above 90 degrees. Tears in this muscle usually occur in the front of the humerus attachment point.
Infraspinatus muscle; In the area close to its attachment to the humerus, its tendon joins with the supraspinatus tendon.
Teres minor muscle; While its upper fibers end by mixing with the rotator cuff, its lower fibers attach directly to the humerus. Its function is to rotate the arm externally and bring it closer to the body.
Another important structure in the inner layer is the long head of the biceps muscle. The long head of the biceps passes through the shoulder joint and attaches to the upper part of the structure called the labrum. The labrum is a tissue that surrounds the glenoid. A SLAP lesion occurs when the part of the labrum to which the long head of the biceps attaches is separated from the glenoid. This is a disorder that can be treated with the arthroscopic method.
What are the Causes of Shoulder Pain?
According to studies, shoulder pain is the third most common reason for admission to orthopedic clinics, after waist (lomber) and knee pain. The most common complaints about shoulder-related problems are; limitation of movement, loss of strength, instability (dislocations), deformity, and a feeling of crackling at the shoulder joint.
The duration, location, degree and aggravating factors of the complaint have an important place in making the diagnosis. While pain at rest indicates diseases such as impingement syndrome and frozen shoulder, pain occurring when the arm is raised above the head may be due to shoulder fiber tears (rotator cuff tears). If the pain extends to the lower parts of the elbow or is accompanied by numbness, it may be related to a cervical disc herniation. Again, in cases of calcific tendinitis and shoulder joint arthritis, pain is observed at rest and at night.
Pain, loss of strength and limitation of movement may occur together in shoulder fiber tears (rotator cuff/cuff tears), for which we frequently perform closed surgery.
Shoulder Fiber Tears (Rotator Cuff / Cuff Tears)
Rotator cuff problems are the most common cause of shoulder pain. Rotator cuff problems occur in a wide range. This can range from simple overuse to impingement syndrome, partial (half) tear, full thickness tear, and rotator cuff arthropathy (calcification), which occurs in the advanced stages when the full thickness tear is not treated.
The rotator cuff consists of 4 muscles. These; supraspinatus, infraspinatus, teres minor and subscapularis. A tear is usually seen in the supraspnatus muscle tendon. The supraspinastus muscle is one of the main muscles that allows us to open the arm laterally.
In cases of rotator cuff problems such as overuse, impingement syndrome and partial tear, medication and physical therapy can be applied first. If the patient does not benefit from these treatments, surgical procedures are applied. However, if there is a full-thickness tear, it is usually always treated with surgery first. Surgical methods can be divided into two: open and closed techniques (arthroscopic). In recent years, with the development of techniques, the arthroscopic surgical method, which is more comfortable for the patient, has begun to be used more frequently.
If rotator cuff tears are not treated, cuff arthropathy (shoulder joint cartilage damage) will develop in the future. This is a condition characterized by arthritis in the shoulder joint. All shoulder movements of the patient become painful.
The treatment is shoulder prosthesis. Therefore, patients with muscle tears around the shoulder should be treated as soon as possible.
Rotator cuff tears are divided into 4 according to their size:
- Small: less than 1cm,
- Medium: between 1 and 3 cm,
- Large: between 3 and 5 cm,
- Massive: Contains tears larger than 5 cm.
How Does Shoulder Fiber Tear Happen? / What Causes Shoulder Fiber Tear?
If there is a tear in the rotator cuff, it usually occurs in the supraspinatus muscle. A tear can occur with shoulder trauma. Another reason is considered to be decreased vascularity.
Above the supraspinatus muscle (the most frequently torn rotator cuff muscle), there is the epaulette bone (acromion), and below it is the upper arm bone (humerus). The muscle moves between these two bones. In some people, the epaulette bone (acromion) has a hook-shaped extension extending downwards. This is called Type III Acromion. The supraspinatus muscle becomes compressed between the acromion and the humeral head, and then tears begin to form. Since there will be more compression in people with hook-shaped acromions, shoulder fiber tears are more common in these people.
Another reason is that rotator cuff tissue quality deteriorates with age and this area is exposed to mechanical loads for many years.
Who Gets Shoulder Fiber Tear (Rotator Cuff / Cuff Rupture)?
It is especially seen in middle-aged and elderly patients. This is because this area is exposed to mechanical loads for a long time and the rotator cuff tissue quality degenerates over time. At the same time, studies have shown that the hook-shaped acromion (epaulette bone) increases more with age. This situation causes compression of the shoulder fibers and paves the way for tears.
How to Diagnose Shoulder Fiber Tear (Rotator Cuff / Cuff Rupture)?
In diagnosis, history and examination are the primary and most important steps. During the examination, some tests are performed to identify shoulder pathologies. If a tear is suspected, imaging methods are used. X-ray is the most frequently used imaging method by orthopedists. X-ray examination may be sufficient in patients with no obvious examination findings and have an innocent history. But this constitutes a small group.
Generally, patients with shoulder pathology will need to undergo MRI. The definitive diagnosis is made after MRI. It is possible to fully evaluate the rotator cuff muscles with MRI. We can distinguish the tear type and size. MRI helps us greatly in determining our treatment method.
What is the Treatment for Shoulder Fiber Tear? (What is the Treatment for Rotator Cuff Rupture?)
Treatment can be non-surgical or surgical. Shoulder fiber tears occur in a wide range, ranging from a simple compression to a full-thickness tear. Therefore, treatment varies from person to person. There are two main purposes in treatment; to relieve pain and restore the loss of function. Treatment also varies depending on the type and size of the tear. Simple tears and impingement cases in the initial stages can be treated with medication and exercise, while injections into the shoulder joint can be performed in more advanced stages. In patients who do not benefit from these treatments or who are in more advanced stages, it is necessary to repair the torn fiber with surgery.
What Happens If Shoulder Fiber Tear Is Not Treated? (What Happens If Rotator Cuff Rupture Is Not Operated?)
The disease is expected to be progressive in untreated patients. The patient presenting with impingement will progress to a half tear in the next stage. A half (partial, not full thickness) tear can later turn into a full thickness and massive tear. A disease that can initially be treated with simple exercises and medication may turn into surgery. If a full-thickness and/or massive tear is not treated, the shoulder joint will develop arthritis (arthrosis). After arthrosis (calcification) develops, the treatment to be performed is shoulder prosthesis.
How is Shoulder Fiber Tear (Rotator Cuff / Cuff Rupture) Surgery Performed?
It is possible to roughly divide surgeries into two as open and closed surgeries. In the past, only cleaning surgery called debridement was performed without repairing. Today, it can still be applied to tears that cannot be repaired.
Repair with open surgery; has been used for many years. In some cases, repair can still be performed with open surgery.
Repair with mini open method; It has begun to be used as an alternative to open surgery. There are orthopedic surgeons who use this method.
Completely arthroscopic (closed) repair; Its use has gradually increased with the development of technology. It has many advantages. Today, it can be considered the most effective method in the treatment of fiber tears.
Closed (Arthroscopic) Shoulder Fiber Tear Surgery
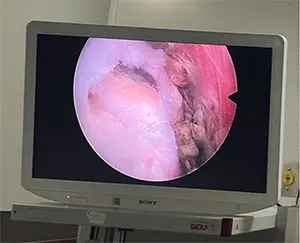
First, the tear type, shape and size should be determined. During the surgery, small incisions are made around the shoulder. These are called portals. The surgery is performed through these pots. Special camera systems, hand tools, special orthopedic implants and sutures are used.
On the screen using an arthroscopic camera shoulder fiber tear displayed.
Shoulder fibers repaired by arthroscopic (closed) method.
When Can I Use My Arm After Closed (Arthroscopic) Shoulder Fiber Tear Surgery?
A good rehabilitation program is needed to contribute to the recovery process after surgery, to ensure return to functional activities and to improve quality of life. When to start using the arm depends on the type and size of the tear. In partial and small tears, the arm can be mobilized earlier, while in advanced massive tears, the time may be longer. This period usually varies between 3 and 6 weeks.
Shoulder Dislocation (Shoulder Joint Instability)
We can group instability under 4 headings. TUBS (traumatic, unilateral, bankart, surgery), AMBRİ (atraumatic, multidirectional, bilateral, rehabilitation, inferior capsular shift), AIOS (acquired, instability, overstressed shoulder) and voluntary instability. Shoulder dislocation is a condition that usually occurs as a result of trauma and is treated surgically.
Recurrent dislocations, especially after the first dislocation, are a strong indication for surgery. The surgery is successfully performed closed by the arthroscopic method. The shoulder joint usually dislocates anteriorly as a result of trauma, causing the lower front part of the structure we call the labrum to rupture. This is called Bankart lesion. Repairing the Bankart lesion prevents recurrent dislocations of the shoulder. Special tools and ropes are used during Bankart repair.
Bankart lesion is seen in 90% of first shoulder dislocations. With the development of techniques in the last 20-30 years, arthroscopic shoulder dislocation treatment has begun to be widely applied. Studies have shown that after the first dislocation, there is a recurrence rate of up to 90% in people under the age of 20. This rate is 15% in people over the age of 40. Our main goal after surgery is to prevent recurrent shoulder dislocation.
What are the mechanisms of shoulder dislocation?
The shoulder usually dislocates as a result of trauma. Most of the time, it projects towards the front-bottom side. Some people are structurally more prone to shoulder dislocation. These; Examples include people with ligament laxity or a small glenoid (the surface on which the shoulder joint sits) area.
Shoulder dislocation can also occur in people who have electric shocks and epileptic seizures. Posterior shoulder dislocation (dislocation of the shoulder joint backwards) should definitely be considered, especially in patients who present with shoulder complaints after an epileptic seizure.
What is the Treatment for Shoulder Dislocation?
The first emergency treatment for shoulder dislocation is to replace the shoulder joint dislocation. The shoulder joint can be repositioned with or without anesthesia. Very rarely, if shoulder dislocations do not settle under anesthesia, urgent surgical treatment is required.
My Shoulder Dislocated and Then They Fixed It, What Happens Now?
First of all, it is recommended to keep the arm in a shoulder arm sling or velapu bandage for a while (usually 2 weeks).
In normal people, after a traumatic dislocation of the shoulder joint, the labrum structure, which has an important role in keeping the shoulder joint in place, is torn. Usually, the anterior and inferior labrum are torn as the shoulder dislocates forward and downward. This injury is called Bankart lesion. Especially in the young population, the likelihood of recurrent dislocations after the first dislocation is higher. Recurrent dislocations can cause irreversible damage to the shoulder joint cartilage.
Taking into account the patient's age, activity status and expectations, the Bankart lesion is repaired with closed surgery after dislocation. After the repair, the shoulder will not dislocate due to simple trauma.
What Happens If I Don't Have Shoulder Dislocation Surgery?
Surgery is strongly recommended at a young age, for simple traumas after the first dislocation, and for recurrent dislocations. In the long term, there may be irreversible damage to the shoulder joint. Since cartilage damage may develop, the possibility of shoulder pain in the future increases.
How Does Shoulder Dislocation Surgery Happen?
The main purpose of the treatment after shoulder dislocation is to prevent the shoulder from dislocating again due to simple traumas and to regain functional shoulder joint movements. After shoulder dislocation, the labrum structure is torn. The procedure performed in surgery is to repair the labrum. Closed (arthroscopic) surgical method is now used as the gold standard in labrum repair. With closed shoulder surgery, repair is performed using special camera systems and special orthopedic implants.
How many hours does closed shoulder surgery take?
The duration may vary depending on the patient and the surgeon performing the operation. During shoulder arthroscopy, different procedures can be added to the operation according to the patient's needs. The time may take longer time depending on the procedure performed. The average time for closed shoulder surgeries is 1 hour.
What is the recovery process like after closed shoulder surgery?
Patients can start light rehabilitation the day after the operation. A shoulder bandage is used for approximately 3-4 weeks. It takes an average of 4 weeks to return to daily life. It takes an average of 2 months for the patient to return to an active life and be able to do sports.
Is there pain after closed shoulder surgery?
The pain scale varies depending on the patient's pain threshold and surgical wound areas. Depending on the procedures performed in the surgical area, the most severe pain occurs in the first 2 days. The pain is expected to gradually decrease in the following days. In general, shoulder pain complaints are expected to disappear completely in the medium and long term.
What are the patient comments after closed shoulder surgery?
After a suitable shoulder arthroscopy, it is expected that the pain will completely disappear and the joint range of motion will be fully restored. The recovery period in open surgery is quite long and painful. Since the procedure we perform is performed in a closed manner (arthroscopic technique), the recovery time is shorter, there is no scar, and the return to daily life is faster. In general, it is an operation with very high patient satisfaction feedbacks.
What are the comments of those who had shoulder surgery?
After a suitable shoulder arthroscopy, it is expected that the pain will completely disappear and the joint range of motion will be fully restored. The pain seen in the first days after the operation is replaced by a feeling of well-being in the following period. Physical therapy started after the pain subsides helps restore full muscle functions, accelerates recovery, and increases patient satisfaction. Closed shoulder surgery is an operation with generally high patient satisfaction.
How are shoulder surgery prices determined?
There are many variables in determining the cost. Selection of an experienced surgical team and use of appropriate materials are essential for the success of the surgery. The price varies depending on the age of the patient, the type of tear, the presence of accompanying injury, and the types and number of materials to be used.